Type 2 Diabetes Treatment Recommendation Tool
This tool helps identify which type 2 diabetes treatment options may be most appropriate for you based on your health profile. It's designed to complement medical advice, not replace it.
Your Health Profile
Your BMI Calculation
Treatment Recommendations
Enter your information above to see personalized recommendations.
Metformin has been the go-to drug for type 2 diabetes for over 60 years. It’s cheap, safe, and works for most people. But if you’re still struggling with blood sugar control, weight gain, or side effects like bloating and diarrhea, you’re not alone. And you might be wondering - is there something better out there now?
The short answer: yes. Several newer drugs outperform metformin in key areas - not because they’re "stronger," but because they do things metformin simply can’t. They don’t just lower blood sugar. They protect your heart. They help you lose weight. They even reduce your risk of kidney failure. And for many patients, they’re now the first choice - even before metformin.
Why metformin isn’t enough for everyone
Metformin works by making your liver less greedy. It stops it from dumping too much glucose into your blood, especially overnight. It also helps your muscles absorb sugar better. Simple. Effective. But here’s the catch: it doesn’t fix the root problems most people with type 2 diabetes face - insulin resistance, fat buildup around organs, and damaged pancreas cells.
Studies show about 30% of people on metformin still can’t reach their HbA1c target of under 7%. And for every 1% drop in HbA1c, your risk of heart disease drops by 14%. So if you’re stuck at 7.8% or 8.2%, you’re still at high risk.
Plus, metformin doesn’t help with weight. In fact, many people gain weight over time - not because of the drug, but because their body keeps fighting to store fat. And if you’re overweight (which most people with type 2 diabetes are), that extra weight makes insulin resistance worse. It’s a cycle.
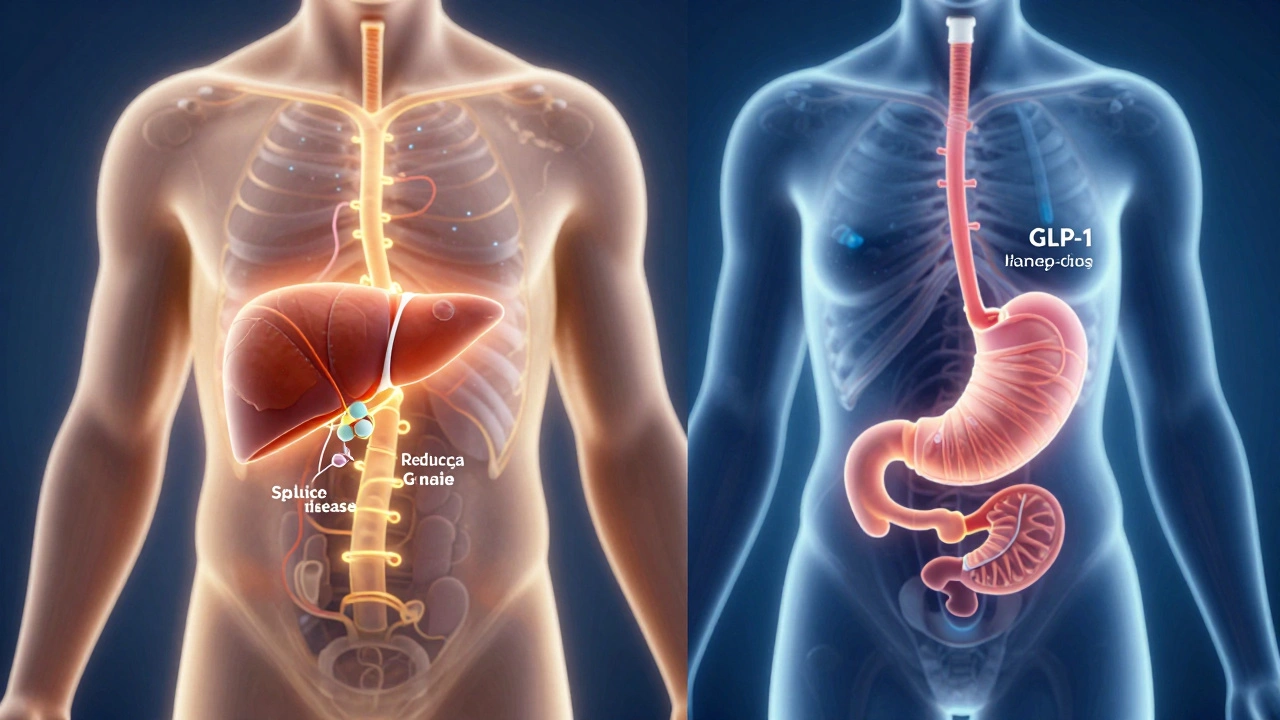
The new generation: GLP-1 agonists
Drugs like semaglutide (Wegovy, Ozempic), liraglutide (Victoza), and dulaglutide (Trulicity) are game-changers. They mimic a natural hormone your gut makes after eating - GLP-1. This hormone tells your pancreas to release insulin only when blood sugar is high. No guessing. No crashes.
But the real magic? These drugs slow down your stomach. You feel full faster. You crave less sugar. You eat less. And you lose weight - on average, 10 to 15% of your body weight over a year. That’s not a side effect. That’s the point.
A 2024 study in The New England Journal of Medicine tracked 8,000 people with type 2 diabetes and heart disease. Those on semaglutide had a 26% lower risk of heart attack, stroke, or death from heart problems than those on placebo. And they lost 12 pounds more on average.
These aren’t just "add-ons." In 2023, the American Diabetes Association updated its guidelines to say GLP-1 agonists should be considered first-line for people with diabetes who also have heart disease, kidney disease, or obesity.
SGLT2 inhibitors: The kidney-saving class
Another group of drugs - SGLT2 inhibitors like empagliflozin (Jardiance), dapagliflozin (Farxiga), and canagliflozin (Invokana) - work differently. They tell your kidneys to throw out extra sugar through urine. It’s like installing a leak in the system so sugar doesn’t build up.
That means you lose 2 to 5 pounds just from flushing out sugar. But the bigger win? These drugs cut your risk of hospitalization for heart failure by 30% and slow kidney disease progression by up to 40%. For people with early kidney damage (microalbuminuria), this can mean avoiding dialysis.
One 2025 trial followed 6,000 patients with type 2 diabetes and chronic kidney disease. Those on dapagliflozin were 39% less likely to reach end-stage kidney disease over 4 years. That’s not just managing diabetes. That’s saving organs.
And unlike metformin, these drugs work even if your kidneys are already a little damaged. Metformin gets pulled if your kidney function drops below a certain level. SGLT2 inhibitors? They’re often the first choice when kidney disease is present.
What about other options?
There are older drugs like sulfonylureas (glimepiride, glyburide) and thiazolidinediones (pioglitazone). But they’re rarely used anymore. Sulfonylureas force your pancreas to pump out insulin - even when it’s not needed. That leads to low blood sugar episodes and weight gain. Pioglitazone can cause fluid retention and bone fractures.
Then there’s insulin. Yes, it works. But it’s not a "better" drug than metformin - it’s a last resort. Insulin requires injections, careful dosing, and constant monitoring. It often causes weight gain. And if you’re not disciplined, it can lead to dangerous lows.
For most people, the goal isn’t to replace metformin with insulin. It’s to replace it with something smarter - something that doesn’t just lower sugar, but fixes the underlying damage.
Who gets these new drugs first?
Not everyone. Cost and access still matter. In India, GLP-1 agonists can cost ₹15,000 to ₹25,000 per month. SGLT2 inhibitors are slightly cheaper - around ₹8,000 to ₹12,000. Metformin? ₹20 to ₹50 a month.
But here’s what doctors are seeing: people who start on semaglutide or dapagliflozin often end up spending less overall. Why? Fewer hospital visits. Less need for dialysis. Lower risk of amputations. Fewer heart attacks.
So while metformin is still the starting point for many, doctors are now asking three questions before prescribing:
- Do you have heart disease or high risk?
- Do you have kidney damage or high urine protein?
- Are you overweight (BMI over 27)?
If you answered yes to any of these - you’re likely a candidate for a GLP-1 agonist or SGLT2 inhibitor before adding metformin.
Can you take them together?
Absolutely. In fact, that’s becoming standard. Many patients now take metformin + a GLP-1 agonist. Or metformin + an SGLT2 inhibitor. Or even all three.
Metformin handles liver glucose. The GLP-1 drug controls appetite and insulin timing. The SGLT2 inhibitor flushes out extra sugar through the kidneys. Together, they cover the whole system. And studies show this combo reduces HbA1c by 2 to 2.5 percentage points - more than any single drug.
Side effects? Mostly mild. Nausea with GLP-1 drugs fades after 2-4 weeks. Urinary tract infections with SGLT2 inhibitors are rare and easy to treat. Neither causes low blood sugar when used alone.
What’s next?
The next wave? Dual agonists. Drugs like retatrutide (still in trials) that hit three receptors at once - GLP-1, GIP, and glucagon. Early results show 20% weight loss and HbA1c drops of 3%. That’s not just treatment. That’s reversal.
And in places like Bangalore, where over 1 in 5 adults have diabetes, the shift is already happening. Clinics are moving away from "just take metformin" to personalized plans: heart first, kidneys second, weight third.
Metformin isn’t obsolete. But it’s no longer the whole story. The best drug for type 2 diabetes today isn’t the cheapest one. It’s the one that protects your heart, saves your kidneys, and helps you live better - not just survive.
Is metformin still the best first drug for type 2 diabetes?
For many people, yes - especially if they’re young, lean, and have no heart or kidney issues. But if you have obesity, heart disease, or early kidney damage, newer drugs like GLP-1 agonists or SGLT2 inhibitors are now recommended as first-line options. Guidelines changed in 2023 to reflect this.
Do GLP-1 drugs cause low blood sugar?
No, not when taken alone. GLP-1 agonists only trigger insulin release when your blood sugar is high. That’s why they rarely cause hypoglycemia. But if you’re also on insulin or sulfonylureas, your risk goes up. Always check with your doctor before combining drugs.
Can I stop metformin if I start a newer drug?
Sometimes. Many patients do well on a GLP-1 or SGLT2 inhibitor alone. But others need metformin to keep liver glucose in check. Your doctor will decide based on your HbA1c, weight, and how your body responds. Never stop metformin without medical advice.
Are these new drugs available in India?
Yes. Semaglutide, dulaglutide, empagliflozin, and dapagliflozin are all approved and available in India. Generic versions of SGLT2 inhibitors are now priced under ₹5,000/month. GLP-1 drugs are still expensive, but patient assistance programs exist through some hospitals and pharma companies.
How long does it take to see results from GLP-1 or SGLT2 drugs?
Blood sugar starts dropping in 1-2 weeks. Weight loss with GLP-1 drugs usually begins after 4-6 weeks and continues for 6-12 months. Kidney protection from SGLT2 inhibitors shows up in urine tests within 3 months. Consistency matters more than speed.